
Severe Demyelination in Non-MS Patient After TNF-α Blocker Treatment Detailed in Study
Written by |
TNF-α blocking drugs, such as infliximab, surprised investigators when their use in people with multiple sclerosis (MS) actually triggered demyelination. In a case report published in the journal Neuroimmunology & Neuroinflammation, Vanderbilt University Medical Center researchers reviewed an aggressive demyelinating event in a non-MS patient treated with TNF-α blockers.
TNF-α blockers are used to slow the progression of autoimmune diseases with an inflammatory component, such as inflammatory bowel disease (IBD) and rheumatoid arthritis (RA). Based on positive treatment results in both patient groups, clinical trials of drugs targeting TNF-α signaling in multiple sclerosis (MS) patients were commenced — and prematurely shut down. MS patients reacted to the drugs with earlier and more frequent exacerbations, and TNF-α blockers were contraindicated for the disease.
Demyelinating events in people with no previous MS-related history have also been reported in scientific journals. The pathological findings in these patients, upon clinical, laboratory, and radiographic review, resemble MS pathological patterns. The death of the patient presented in this case study allowed for a histological confirmation of demyelination following TNF-α blocker treatment.
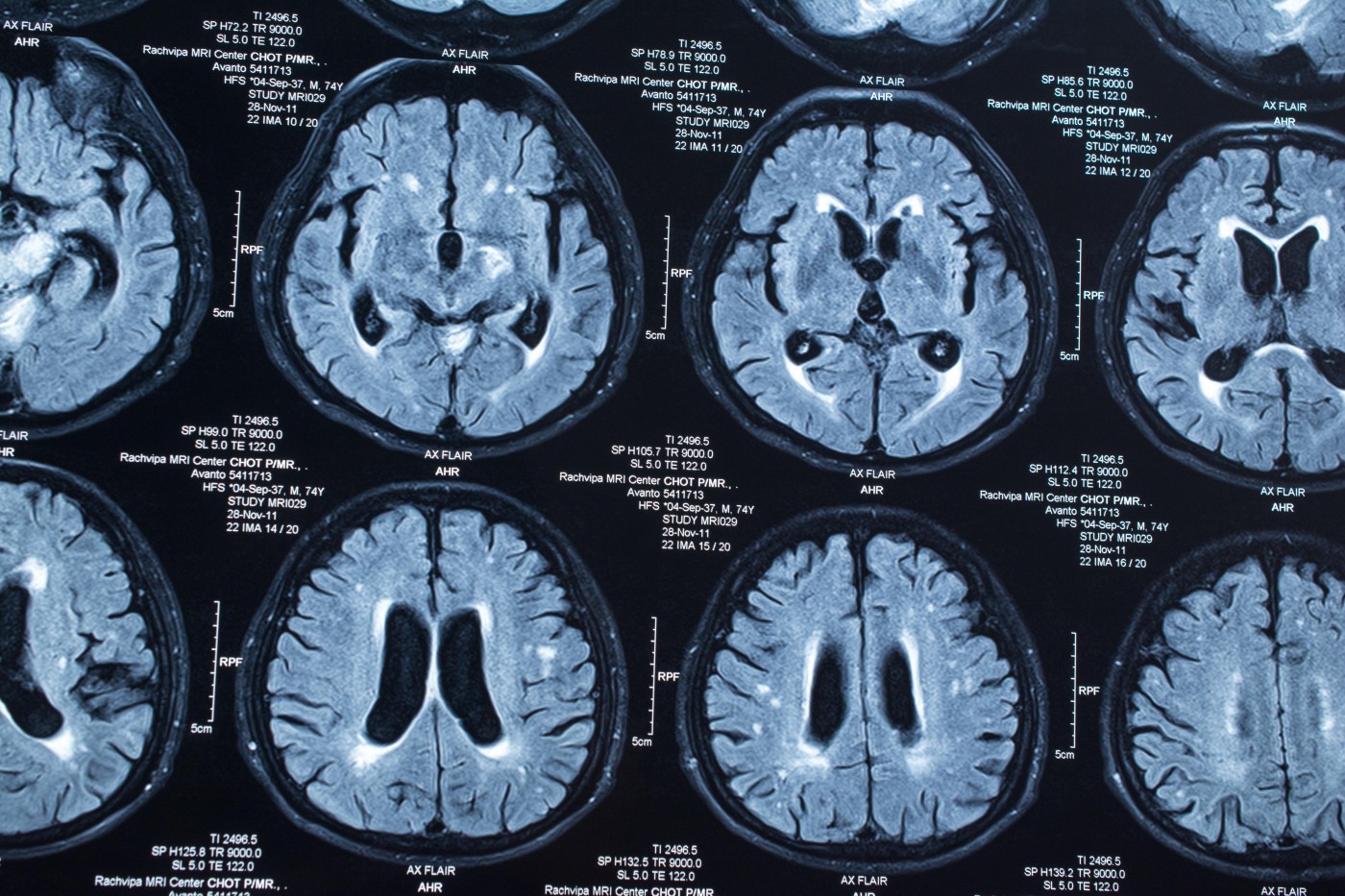
As reported in “Autopsy-Proven Demyelination Associated With Infliximab Treatment,“ a 57-year-old man treated with TNF-α blockers for four months arrived at a hospital with obvious deterioration in brain function, including facial weakness and ataxia. He had also developed a rash. Brain magnetic resonance imaging (MRI) scans showed lesions suggestive of demyelination in the brainstem and in parts connecting the brain stem with the cerebellum. Lesions in deep brain structures, such as the striatum, and in superficial cortical tissue were also found.
Clinicians could find no support for a microbial cause to the brain lesions, and a biopsy of the rash suggested autoimmune mechanisms, toxicity, or hypersensitivity reactions, or disease caused by virus or the bacteria Rickettsia.
The lesions progressively worsened. Although the man had initially responded to aggressive steroid treatment, he died following a multi-drug-resistant infection with Klebsiella pneumoniae. A brain autopsy confirmed a process of acute demyelination, mainly involving white matter.
Previous studies on demyelination following TNF-α treatment present with various clinical signs of demyelination as well as skin reactions, the authors noted. In most patients, neurological complications are reversed upon cessation of TNF-α blockers, but an estimated 25 percent develop MS despite discontinuation.
Researchers are still in the dark about how TNF-α blockers cause demyelination. Several mechanisms have been suggested, such as the possibility that prolonged exposure to TNF-α antagonism increases the immune T-cell response or alters the cytokine profile — events that could favor demyelination. These are, however, only hypotheses and scientists are still searching for the cause of TNF-α treatment-related MS.
Shasha
Blood tests may not work to diagnose low Vit B12.They maybe very low, but blood tests say they are alright. People may not get Vit B12 methylcobalamin shot/spray/under the tongue kind/cream/intrinsic factor kind which can remyelinate the brain. TNF-α blockers may lower the immune system allowing Lyme/other infections to grow which may demyelinate the brain. Maybe it interfers with Vit D etc. Anything that lowers oxygen like swelling may demyelinate the brain. He got steriods which may hurt the liver. I would have to research it more. Too bad. Fish oil helps the brain/immune system and MS people. Vit C may help the immune system. To bad it is used for anyone. Celiac help instead may help.
Lori Batchelor
I was in the clinical trial on MS patients mentioned in1996--"clinical trials of drugs targeting TNF-α signaling in multiple sclerosis (MS) patients were commenced — and prematurely shut down. MS patients reacted to the drugs with earlier and more frequent exacerbations, and TNF-α blockers were contraindicated for the disease."--they've known TNF causes demyelination since 1996!
Erik Visser
I am a man, born in 1957. In 2006 I was treated with Enbrel (Etanercept), a TNF-a blocker, for Ankylosing Spondylitis. (Bechterew disease). After 5 months I had several deficits, most in my face and jaw and lost my taste. I stopped using Enbrel but the deficits got worse. Three months and 2 MRI’s later I was diagnosed Multiple Sclerosis.
Lori Batchelor
Sorry to hear that..I would have thought they had learned how dangerous demyelination is after the study I was in...
olly
what study?
molly
I am 34 I was treated with Enbrel for 4 weeks and lost feeling in the right side of my face, left side fine weakness and fine motor function, terrible exhaustion, numbness in my leg. They said it was the demyelination but here I am 5 months later and still having symptom flare ups. I just went for a follow up scan to see if I have more lesions on my brain and they said may be MS. I have been battling this with no answers all they did was pump me up on 80mg of prednisone a day and when I stop it I get all the symptoms back. I just want answers!
oswaldo salcedo
...very oversimplified writing, read this one
"These important findings in pre-clinical models have clinical implications and suggest that inhibition of tmTNF/TNFR2 signaling by lenercept was the molecular basis for the worsening symptoms in MS patients. Experiments to block solTNF/TNFR1 signaling with the solTNF-selective DN-TNF inhibitors in the cuprizone model should yield further support for this hypothesis. Transgenic animal models in which tmTNF is expressed exclusively demonstrated that tmTNF, in the absence of solTNF, suppresses EAE disease onset and progression, while still maintaining the ability of TNF signaling to suppress autoimmune properties.[134,135] This ability of tmTNF to maintain immune functions such as self-tolerance and resistance to infection while limiting other TNF functions including primary demyelination and oligodendrocyte apoptosis[135] opens the possibility of selective inhibition of solTNF/TNFR1 signaling as a therapeutic strategy to prevent relapsing-remitting MS in patients afflicted with this chronic inflammatory disease of the nervous system"
Kassiotis G, Kollias G: Uncoupling the Proinflammatory from the Immunosuppressive Properties of Tumor Necrosis Factor (TNF) at the p55 TNF Receptor Level: Implications for Pathogenesis and Therapy of Autoimmune Demyelination. J Exp Med 2001, 193:427-434.
Jackie
In the absence of any alternative for inflammatory arthritis, anti tnfs are still a godsend for most of us. We know the risks.
Noel
I would rather live to walk my daughter down the aisle in pain than die when she is in 9th grade and been able to run a marathon. The FDA needs to do their job
L
My son had a dose of Remicade and it didn't help his Ulcerative Colitis so they did surgery, a day or two later. They shouldn't have given him the dose if they knew that surgery was inevitable anyway. So, now he is having "flares" of itching all over his body. It's been going on for several months and the Remicade was given in June 2018. He is scheduled to see a neurologist but the appointment is about a month away. Is this possibly MS, after Remicade?