Copaxone (glatiramer acetate injection) for multiple sclerosis
Last updated July 24, 2025, by Lindsey Shapiro, PhD
 Fact-checked by Inês Martins, PhD
Fact-checked by Inês Martins, PhD
What is Copaxone for MS?
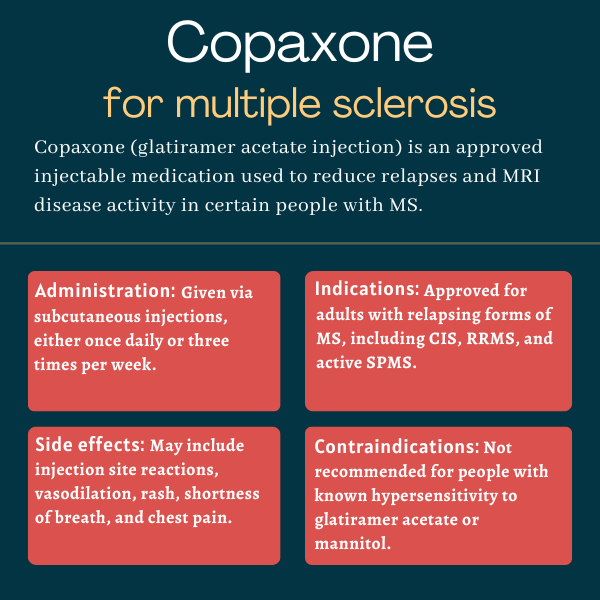
Copaxone (glatiramer acetate injection) is an approved therapy for adults with relapsing forms of multiple sclerosis (MS), including clinically isolated syndrome (CIS), relapsing-remitting MS (RRMS), and active secondary progressive MS (SPMS).
Given via subcutaneous (under-the-skin) injections, this disease-modifying treatment helps reduce relapses and lesions, and there is evidence that it may also delay disability progression.
The active ingredient in Copaxone is glatiramer acetate, a lab-made molecule designed to mimic a protein found in myelin, the fatty substance that surrounds and protects nerve cells and which is progressively lost due to erroneous immune attacks in MS. Exactly how it works is poorly understood, but Copaxone is broadly thought to modulate the activity of immune cells that are responsible for these inflammatory attacks, and to directly act on nerve cells to protect them against damage.
The brand-name medication is marketed by Teva Pharmaceuticals, but several generic versions are also widely available.
Therapy snapshot
| Brand name: | Copaxone |
| Chemical name: | Glatiramer acetate |
| Usage: | Used to reduce disease activity in relapsing forms of MS |
| Administration: | Subcutaneous injection |
Who can take Copaxone?
Copaxone is approved in the U.S. for treating adults with CIS, RRMS, and active SPMS.
The medication is contraindicated for people with a history of hypersensitivity (harmful immune responses, including allergic reactions) to glatiramer acetate or mannitol, one of the therapy’s inactive ingredients. Copaxone carries a boxed warning for anaphylaxis, a type of severe allergic reaction that can affect the airways and be life-threatening or fatal.
Copaxone is similarly approved in more than 50 countries worldwide, including the European Union and Canada.
How is Copaxone administered?
Copaxone comes in single-dose, prefilled syringes and is administered via subcutaneous injections in either of two dosing schemes:
- 20 mg/mL, once per day
- 40 mg/mL, three times per week and at least 48 hours apart
The injections are done in areas such as the arms, abdomen, hips, and thighs, and injection sites should be rotated. The first dose is given under the guidance of a healthcare professional, but patients can self-administer Copaxone after receiving proper training. An optional compatible autoinjector device is available to help with injections.
Copaxone in clinical trials
Approvals for both dosing regimens of Copaxone were backed by a number of Phase 3 trials.
- A trial conducted in the 1990s at several U.S. sites supported the initial approval of the 20 mg daily dosing regimen. Data showed that Copaxone led to significant reductions in relapses after two years compared with a placebo among adults with RRMS. People on Copaxone were also significantly more likely to experience an easing of disability, while those on the placebo were more likely to experience worsening disability.
- Two other placebo-controlled studies similarly tested the 20 mg daily dosing regimen in people with RRMS. Findings from these trials also demonstrated Copaxone’s ability to reduce relapses and lower MRI disease activity in this population.
- The PreCISe trial (NCT00666224) compared the 20 mg dose with a placebo in 481 patients with CIS. Data showed that daily Copaxone significantly lowered the risk of progression to clinically definitive MS after three years.
- The 40 mg thrice-weekly dosing regimen was backed by data from a Phase 3 trial called GALA (NCT01067521), which enrolled 1,404 RRMS patients worldwide. Data showed that this regimen had a similar safety and efficacy profile to the original formulation, and follow-up data at seven years showed that patients who received the higher dosage from the main trial continued to have lower relapse rates than those who first received a placebo.
Findings from an open-label extension study that followed patients for up to 27 years on continuous Copaxone have generally indicated that the benefits are sustained long-term, and that starting treatment early was linked to a lower rate of relapses and a delay in confirmed disability worsening.
Common side effects of Copaxone
The most common side effects associated with Copaxone in clinical trials include:
- injection site reactions
- vasodilation, or a widening of blood vessels that can cause blood pressure to drop
- rash
- shortness of breath
- chest pain, which is usually temporary.
Copaxone also carries a boxed warning noting it can cause anaphylaxis, a rare but serious allergic reaction that can be fatal. These reactions can occur at any time, from as early as the first dose to up to years after treatment initiation. Patients should be advised by their prescribing doctor of the possible symptoms of anaphylaxis, which may overlap with those of immediate post-injection reactions. If these symptoms occur, patients should seek immediate medical care and treatment with Copaxone should be immediately stopped.
Other serious side effects that may occur while on treatment with Copaxone include:
- immediate post-injection reactions
- subcutaneous fat loss or skin cell death at injection sites, which can be avoided with proper injection techniques
- altered immune responses
- liver injury, which may require treatment discontinuation.
Multiple Sclerosis News Today is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
FAQs about Copaxone
Copaxone was initially approved by the U.S. Food and Drug Administration in December 1996 for the daily treatment of adults with relapsing-remitting multiple sclerosis (MS). The label was later expanded to also include other forms of relapsing MS. A different formulation of the medication that’s injected less frequently was approved in 2014.
According to animal data and findings from observational clinical studies, Copaxone use during pregnancy does not harm a developing fetus. However, there haven’t been any well-controlled studies in pregnant women. Patients are advised to inform their healthcare team if they are pregnant or have plans to become pregnant while on Copaxone.
No known interactions exist between Copaxone and alcohol. However, given that alcohol can interfere with some medications and disease symptoms, patients should discuss the topic with their healthcare providers.
According to Copaxone’s developer, Teva Pharmaceuticals, patients using the medication may see results after one year. However, responses to treatment can vary. Patients should talk with their healthcare team about how Copaxone is expected to help in their case.
Weight gain and hair loss were not reported in clinical trials as common side effects of Copaxone, but there are some isolated reports of weight gain or weight loss. Patients who experience unanticipated effects from treatment should discuss them with their healthcare team.