
Case Study Highlights Demyelinating Lesion in Pediatric MS Patient Discovered After Abdominal Pain
Written by |
Considering the range of neurological symptoms normally associated with adult multiple sclerosis (including loss of coordination, weakness, fatigue, and trouble thinking), symptoms of pediatric multiple sclerosis are often nonspecific and affect the intestinal system. Intestinal mobility and sensation, vomiting, and long transit time for digestion (dysphagia) are symptoms that also present with demyelination in the central nervous system. Abdominal pain is usually not among these symptoms, but for one seven-year-old child, the only symptom of a new demyelinating lesion was severe abdominal pain.
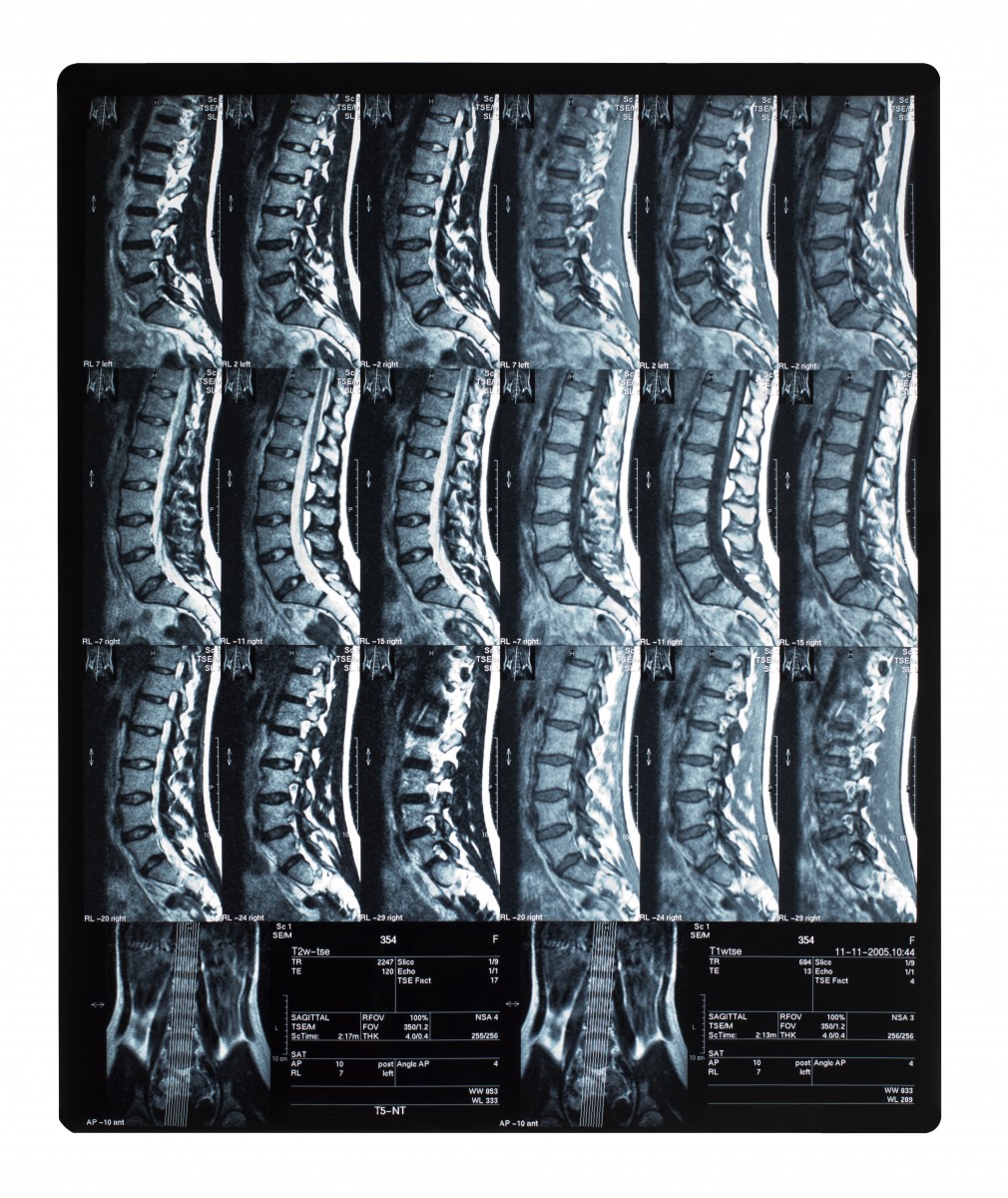
As described in the case study, “Acute Abdominal Pain as the Only Symptom of a Thoracic Demyelinating Lesion in Multiple Sclerosis,” which was published in the journal Brain and Development, the child had a new demyelinating lesion that showed up between thoracic vertebrae T4 and T12. Earlier in his life, the boy had his first symptom of multiple sclerosis at three years of age. At that time, he had spastic gait and was treated with intravenous methylprednisolone (m-PSL). Although he continued to have slight spasticity in both his ankle joints, his symptoms were greatly improved.
Later on in life at age six, the boy had a second symptom of multiple sclerosis. He appeared at the doctor due to neck and upper extremity pain and was officially diagnosed with multiple sclerosis. A more aggressive means of treatment included interferon-beta 1a (IFN β 1a) and plasmapheresis in addition to m-PSL. Treatment with IFN β 1a was eventually stopped because the boy had frequent episodes of vomiting and poor eating, both of which cleared up one month after stopping IFN β 1a treatment.
With the newest multiple sclerosis relapse, the boy was successfully treated again with m-PSL and IFN β 1b (rather than IFN β 1a) as a disease modifying therapy. Remarkably, there was a reduction in the demyelinating lesion with the end of treatment, as well as a resolution of symptoms after three weeks.
“This case is remarkable in that the only symptom of a longitudinally extensive, thoracic, demyelinating lesion was abdominal pain,” commented Dr. Shohei Nomura, lead author of the case study. “Though it is unclear why the only manifestation of this patient’s extensive thoracic lesion was abdominal pain, this case supports the notion that the size and localization of demyelinating lesions might not directly correspond to the symptoms observed. Therefore, clinicians must be careful to consider neurogenic sources of diverse symptoms, especially those related to autonomic dysfunction, in demyelinating diseases such as multiple sclerosis.”


Nina Maggs
It is a sad day when a 2 year old boy is diagnosed with a progressive disease like MS. A cure should be in place not necessarily for the adults who've lived with it for years, but for the children who are diagnosed at a young age, and have their entire lives ruined by this nightmare.
David
The abdominal pain is not a symptom of MS, but rather a symptom of the underlying cause of MS. Gut bacteria is the source of both the abdominal pain and MS, see Eplison Toxin producing Clostridium Perfringens.