Fact-checked by
Fact-checked by 
Transverse myelitis: What is it and how is it linked to MS?
Transverse myelitis and multiple sclerosis (MS) are both inflammatory disorders that cause damage to the nervous system. Usually, people who experience an attack of transverse myelitis will recover and not experience subsequent episodes. But in a minority of patients, transverse myelitis may represent the onset of MS.
What is transverse myelitis?
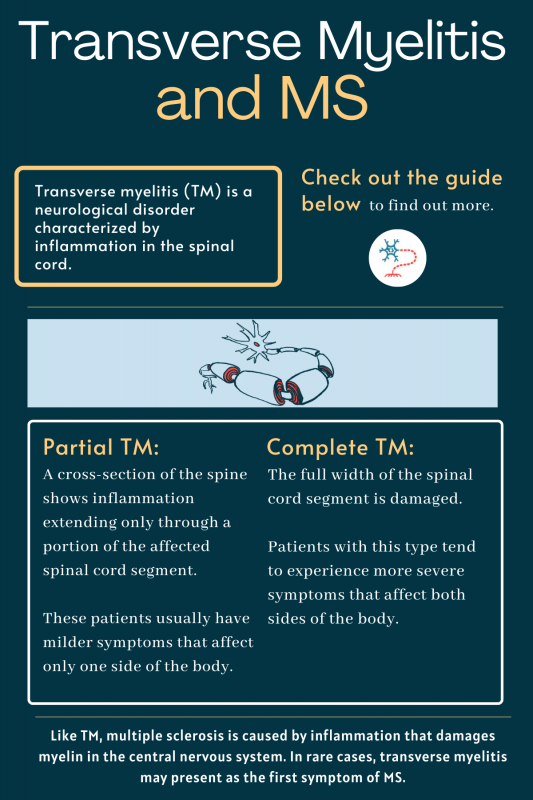
Transverse myelitis, sometimes abbreviated as TM, is a neurological disorder characterized by inflammation in the spinal cord. It is estimated that about 1,400 people in the U.S. are diagnosed with transverse myelitis each year.
The disorder’s name refers to inflammation, so-called “myelitis” that damages myelin, and occurs on both sides — “transverse” — of a segment of the spinal cord. Myelin is a fatty substance surrounding nerve fibers like a sheath, helping them to send electric signals. Loss of myelin, called demyelination, impairs neuronal function and gives rise to disease symptoms.
There are two main types of transverse myelitis:
- partial TM, in which a cross-section of the spine shows inflammation extending only through a portion of the affected spinal cord segment. These patients usually have milder symptoms affecting only one side of the body.
- complete TM, in which the full width of the spinal cord segment is damaged. Patients with this type tend to experience more severe symptoms impacting both sides of the body.
Transverse myelitis and MS
Like TM, multiple sclerosis is caused by inflammation that damages myelin in the central nervous system, comprising the brain and spinal cord. In rare cases, transverse myelitis may present as a first symptom of MS.
Difference between transverse myelitis and MS
MS is defined by inflammation-causing demyelination in multiple parts of the central nervous system at different points in time. By definition, transverse myelitis and MS can be differentiated based on what parts of the nervous system are affected. Specifically, if only a segment of the spinal cord is affected, then a person may be diagnosed with TM. Meanwhile, inflammatory demyelination in the brain, or both the brain and spinal cord, may indicate MS.
Can transverse myelitis turn into MS?
About 5%–10% of people who experience an attack of transverse myelitis will go on to develop multiple sclerosis. In these patients, the initial bout of TM most likely represents a first onset of MS, which causes inflammation in the spinal cord that manifests as transverse myelitis.
The likelihood of developing MS after a transverse myelitis episode generally is greater in people with partial TM, and in those who exhibit demyelinating lesions in the brain.
Among patients with partial TM and evidence of brain lesions on MRI scans, about 80%–90% will develop clinically definite MS within a few years. In contrast, approximately 10%–33% of partial TM patients without brain lesions will go on to develop MS in the following five to 10 years.
Complete TM is more commonly associated with neuromyelitis optica spectrum disorder, another autoimmune condition that damages myelin in the spinal cord and optic nerve.
Symptoms of transverse myelitis
There are four symptoms that are classically characteristic of transverse myelitis:
- weakness in the arms and/or legs, often leading to paralysis
- pain, often in the lower back or as a sharp pain that feels like it is “shooting” through the body
- numbness, tingling, or other abnormal sensations, known as paresthesias
- bladder and bowel problems
These symptoms may appear suddenly, or over the course of hours or days. Usually, after the first symptoms become evident, neurological function tends to continually decline over the course of several days. Most patients reach their worst condition within 10 days, at which point about 50% have completely lost the ability to move their legs, and nearly all exhibit bladder problems.
The majority of people with TM will go on to make a recovery after the initial episode of spinal cord inflammation. Some do experience lingering health problems after an acute attack of transverse myelitis, however.
Risk factors and possible causes of transverse myelitis
Transverse myelitis can affect people of any age, though it most often occurs in youth ages 10 to 19, and in adults in their 30s. There are no associations between TM and gender or family history.
The disease is caused by excessive inflammation or swelling in the spinal cord, often triggered by specific events such as infections, exposure to toxic substances, or injuries. Such events appear to activate the immune system and set the stage for heightened inflammation and spinal cord damage.
Specific conditions linked to TM include:
- autoimmune diseases of the nervous system, including MS, neuromyelitis optica spectrum disorder, and acute disseminated encephalomyelitis
- other autoimmune diseases such as systemic lupus erythematous, Sjögren’s syndrome, and sarcoidosis
- cancer
- vaccines for other diseases, including those against hepatitis B
- viral infections, including herpes viruses and influenza
- bacterial infections, such as syphilis, tuberculosis, tetanus, and Lyme disease
- fungal infections, including those caused by Aspergillus and Cryptococcus genera
- parasitic infestations, such as toxoplasmosis
Still, the exact causes or trigger of transverse myelitis is not known in many cases, even after an exhaustive medical evaluation. These cases are referred to as “idiopathic” transverse myelitis, or of unknown cause.
Diagnosis of transverse myelitis
Diagnosing transverse myelitis generally involves an assessment of a person’s medical history paired with a thorough neurological examination. Specific tests that may be used to diagnose TM, and to rule out other conditions that can result in similar symptoms, include:
- MRI, to image damage in the spinal cord and brain
- CT scan, to look for inflammation in the nervous system
- lumbar puncture, also called a spinal tap, to detect signs of spinal inflammation like increased immune cell counts and protein levels
- a blood test to help rule out other conditions, such as B12 deficiency or infections, or to diagnose underlying autoimmune diseases or cancer
Treatment of transverse myelitis
The standard treatment for transverse myelitis is high doses of anti-inflammatory medications called glucocorticoids, which reduce the inflammation causing damage to the nervous system. These medicines also are used to manage relapses in MS.
Other immune-suppressing medicines, or plasma exchange, may be helpful for treating TM in patients who do not respond well to glucocorticoids. Plasma exchange is a procedure that involves replacing the noncellular portion of blood, which contains antibodies and other toxic molecules that may be contributing to nervous system damage.
In patients with TM that develops due to an infection or autoimmune disease, treating the underlying condition can help to resolve or ease the symptoms of transverse myelitis.
TM patients also may receive additional treatments to manage individual symptoms such as pain. Some individuals may require long-term management and rehabilitation approaches to regain some functional abilities and improve quality of life.
Scroll horizontally to view all columns -->
| Transverse myelitis | Multiple sclerosis | |
|---|---|---|
| Cause | Inflammation on both sides of the spinal cord. Sometimes associated with autoimmune disease or infections | Inflammation that always affects the brain and sometimes the spinal cord |
| Diagnosis | MRI to detect inflammation in the spinal cord | MRI to detect inflammation in multiple parts of the central nervous system at multiple points in time |
| Symptoms | Has four hallmark symptoms:
|
Causes a range of symptoms, including:
|
| Treatment | Treated with anti-inflammatory corticosteroids | Anti-inflammatory corticosteroids to prevent relapses, and disease-modifying therapies to delay disease progression |
| Prognosis | Most patients will recover, though some may have some persisting symptoms. | Patients may have periods of relapse and remission, or may experience gradual symptom worsening over time. |
Life expectancy: Is transverse myelitis fatal?
It is unknown whether transverse myelitis in itself shortens a person’s life expectancy. But the condition can increase the risk of lifelong complications, such as breathing and swallowing issues, that may shorten survival and reduce a patient’s quality of life.
After an acute transverse myelitis episode, most people will experience some degree of recovery. About one-third of patients have a complete or near-complete recovery, with almost all of their symptoms fully gone. Another third or so have a partial recovery, where symptoms ease but don’t entirely disappear.
The other third of patients experience no recovery from their symptoms, and their ability to perform normal day-to-day functions can become permanently affected.
Recovery from transverse myelitis usually starts a few weeks after the initial attack, and the recovery process may take several years. If there is no recovery within the first six months, then any future recovery is unlikely. Patients who experience a rapid onset of severe TM symptoms (e.g., complete limb paralysis) tend to have a worse prognosis.
For those who experience persistent TM symptoms, support such as occupational and/or physical therapy can help make symptoms more manageable. Such therapy also can aid patients in developing strategies for coping in day-to-day life.
People who experience an attack of TM generally do not experience a second subsequent attack. When a second attack does occur, the condition almost always is associated with an autoimmune disease, such as multiple sclerosis or neuromyelitis optica spectrum disorder.
Multiple Sclerosis News Today is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
FAQs about transverse myelitis and MS
Transverse myelitis is considered a rare disease in the U.S., meaning it affects fewer than 200,000 people. Estimates suggest that about one to eight new cases per million people are diagnosed each year in the country. This equates to about 1,400 new cases per year in total. An estimated 33,000 Americans have some disability resulting from transverse myelitis, according to the National Multiple Sclerosis Society.
Transverse myelitis (TM) refers to demyelinating inflammation on both sides of the spinal cord. Sometimes, this inflammation may result from an underlying autoimmune disease like multiple sclerosis or neuromyelitis optica spectrum disorder. However, infections also may precipitate the development of TM. In most cases, the cause of TM is never identified.
Most people with transverse myelitis experience a single acute attack, and recover at least partially from its symptoms. But some patients may experience subsequent disease attacks, with continually worsening symptoms. These cases often are associated with an underlying inflammatory disorder that results in ongoing inflammation and damage to the spinal cord.
The first-line treatment of transverse myelitis generally involves anti-inflammatory medications that reduce the damaging inflammation. Most people will make at least a partial recovery, with symptoms easing after the initial attack. Some patients, however, may experience persistent and debilitating long-term symptoms.
In the vast majority of cases, someone who experiences an episode of TM will not experience subsequent or recurrent transverse myelitis attacks. In the rare cases where a second attack does occur, it usually is accompanied by inflammation elsewhere in the nervous system and indicates the presence of other autoimmune diseases, such as multiple sclerosis.
Related Articles