Guidelines for MS diagnosis: McDonald criteria
Last updated Oct. 13, 2025, by Marisa Wexler, MS
 Fact-checked by Ines Martins, PhD
Fact-checked by Ines Martins, PhD
An early diagnosis of multiple sclerosis (MS) is important but can be complex, as its symptoms often resemble those of other neurological disorders. To help clinicians confirm the disease more accurately and earlier, experts have developed a set of diagnostic guidelines known as the McDonald criteria.
What are the McDonald criteria?
MS is an autoimmune disease in which the immune system mistakenly attacks parts of the central nervous system (CNS), which includes the brain, spinal cord, and optic nerves. This damage disrupts communication between the brain and body, leading to a wide range of symptoms.
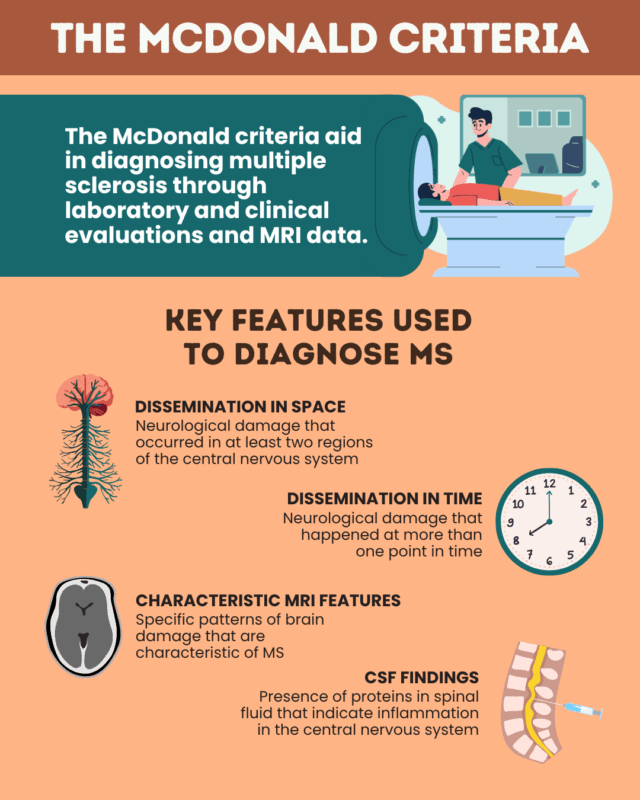
The McDonald criteria are a set of internationally recognized guidelines that incorporate clinical and laboratory evaluations, as well as MRI scans and other tests, to establish an MS diagnosis.
The first version was published in 2001 by an international team led by neurologist Ian McDonald. The criteria have since been updated several times to reflect advances in MS research and imaging technology. The most recent revision took place in 2024.
What features are included in the McDonald criteria?
The 2024 update to the McDonald criteria outlines several scenarios where an MS diagnosis can be established, depending on the patient’s symptoms and test results. To confirm MS, doctors will look for evidence that disease activity has affected the CNS in characteristic ways.
Four main types of evidence can be assessed:
- Dissemination in space: Signs of nerve damage appearing in multiple regions of the CNS.
- Dissemination in time: Evidence that damage has occurred at different points in time.
- Characteristic MRI features: Specific patterns of lesions, such as the central vein sign (CVS) and paramagnetic rim lesions (PRLs).
- Cerebrospinal fluid (CSF) findings: Laboratory evidence of immune activity in the CNS, such as oligoclonal bands (OCBs) or kappa free light chains (kFLCs).
Dissemination in space
Dissemination in space means that nerve damage has occurred in more than one area of the CNS. According to the 2024 McDonald criteria, dissemination in space is demonstrated by the presence of lesions in at least two of five specific CNS regions. These regions include:
- the periventricular, juxtacortical or cortical, and infratentorial regions of the brain
- the optic nerves, which carry visual information from the eyes to the brain
- the spinal cord
In people with gradually worsening MS-like symptoms for at least one year — suggestive of progressive MS — the presence of two or more spinal cord lesions is sufficient to fulfill the criteria for dissemination in space, even if no other regions are affected.
MRI scans of the brain and spinal cord are the main tools used to evaluate dissemination in space. Eye imaging and functional tests, such as optical coherence tomography and visual evoked potentials may also be used to detect optic nerve involvement.
Dissemination in time
Dissemination in time means that neurological damage has happened at more than one point in time. This can be demonstrated by:
- the occurrence of more than one relapse
- the appearance of new lesions on follow-up MRI scans
- clear-cut evidence of brain damage that happened at different times (i.e., new inflammatory lesions alongside older lesions that are no longer actively inflamed)
Characteristic MRI features
Certain MRI findings are highly suggestive of MS and may strengthen diagnostic confidence when used alongside other diagnostic features. These include:
- PRLs, or areas of tissue damage surrounded by a ring of iron-laden immune cells, indicating chronic inflammation. A person with at least one PRL is considered PRL positive.
- CVS, or lesions that contain a small blood vessel at their center. Having at least six lesions with CVS is enough to consider that a person is CVS positive.
Both features are common in MS but rare in other conditions, making them useful in distinguishing MS from other diseases. The 2024 revision formally recognizes that these markers can help support an MS diagnosis in certain situations.
CSF findings
Testing the CSF, or the liquid that surrounds the brain and spinal cord, can provide additional diagnostic evidence. Two key markers characteristically detected in the CSF are:
- OCBs
- kFLCs
The presence of these proteins in the CSF is indicative of abnormal immune activity within the CNS. According to the 2024 McDonald criteria, OCBs and kFLCs can be used interchangeably to demonstrate this inflammation and support an MS diagnosis in certain situations.
How are the McDonald criteria used to diagnose MS?
According to the 2024 McDonald criteria, MS can be diagnosed in people who have typical symptoms of the disease and evidence of any of the following:
- both dissemination in space and dissemination in time
- dissemination in space plus a positive CSF test (OCBs or kFLCs)
- dissemination in space plus CVS positivity
- lesions in at least four of the five regions used to evaluate dissemination in space
If lesions are seen in only one of the five CNS regions in someone with MS-like symptoms, MS can still be diagnosed if one of the following is present:
- a positive CSF test together with MRI signs of CVS or PRLs
- dissemination in time plus evidence of CVS or PRLs
In previous versions of the McDonald criteria, MS could only be diagnosed if patients were experiencing MS-like symptoms. People with MRI findings suggestive of MS but without symptoms were classified as having radiologically isolated syndrome (RIS).
However, under the 2024 update, MS can be diagnosed in some individuals who previously would have been labeled as RIS. Specifically, a diagnosis can be made if patients show dissemination in space and at least one of the following:
- dissemination in time
- a positive CSF test
- CVS positivity
Importantly, the guidelines emphasize that MS should only be diagnosed when no better explanation exists for a person’s symptoms or test results. For that reason, clinicians often perform additional tests to rule out other neurological or inflammatory diseases before confirming an MS diagnosis.
| Presentation | What else is needed to confirm an MS diagnosis? |
|---|---|
| Lesions are found in at least four of the five CNS regions, and the patient is experiencing symptoms indicative of MS | If other potential explanations have been ruled out, MS can be diagnosed without any additional testing |
| Lesions are detected in at least two of the five CNS regions, and the patient is experiencing symptoms indicative of MS | If other potential explanations have been ruled out, MS can be diagnosed if the patient:
|
| Lesions are detected in at least two of the five CNS regions, but the patient is not experiencing any typical MS symptoms | If other potential explanations have been ruled out, MS can be diagnosed if the patient:
|
| Lesions are detected in only one CNS region, but the patient is experiencing symptoms indicative of MS |
If other potential explanations have been ruled out, MS can be diagnosed if the patient:
|
| Lesions are detected in only one CNS region, and the patient is not experiencing any typical MS symptoms | MS cannot be diagnosed unless the patient develops symptoms or additional lesions |
What does the updated version of the McDonald criteria mean for MS patients?
The updated 2024 McDonald criteria, which builds on the previous 2017 revision, do not change or invalidate existing MS diagnoses made under earlier versions. Instead, the update aims to reflect advances in MS research and imaging technology to help clinicians make earlier and more accurate diagnoses, reducing both wait times and the risk of misdiagnosis.
2024 revisions to the McDonald criteria
The 2024 update introduces several important changes from the 2017 version:
- In the previous version, only four areas of the CNS — three brain regions and the spinal cord — could be used to demonstrate dissemination in space. The new version adds the optic nerve as the fifth region that can now be considered.
- Under the old criteria, a diagnosis of MS required evidence of dissemination in time. The 2024 update removes this requirement, allowing MS to be diagnosed in patients with only one clear instance of disease activity, if other supporting evidence is present.
- The new version formally introduces guidance on the use of CVS and PRLs as supporting imaging markers. These findings are highly specific to MS but were not included in prior versions.
- While the earlier version included guidance on the use of OCBs to diagnose MS, the 2024 criteria now include kFLCs as an equivalent biomarker. Because kFLC testing is automated and widely available, it may make diagnosis faster and more consistent across centers.
- Previously, MS could only be diagnosed in people who had typical MS symptoms. The new guidelines allow a diagnosis in asymptomatic individuals who meet other diagnostic criteria, expanding the potential for earlier intervention.
A unified framework for diagnosing all types of MS
One of the most significant changes in the 2024 McDonald criteria is the introduction of a single, unified framework for diagnosing all forms of MS.
Historically, MS has been divided into two broad categories:
- relapsing MS, marked by relapses or flares where symptoms suddenly worsen
- progressive MS, characterized by a gradual worsening of symptoms over time, independent of relapses
Earlier versions of the McDonald criteria used different diagnostic pathways for these forms of the disease. However, growing evidence now shows that relapsing and progressive MS exist on a continuum, with overlapping biological mechanisms and imaging features. The 2024 revision recommends using one consistent approach to diagnose MS, regardless of whether a person’s symptoms appear relapsing or progressive.
The update also eliminates separate diagnostic criteria for adults and children. Instead, it presents a unified set of guidelines applicable to patients of all ages.
Still, the criteria emphasize that clinicians should exercise caution when diagnosing older adults who may have other conditions that can mimic MS, as these can increase the risk of misdiagnosis.
Multiple Sclerosis News Today is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
FAQs about McDonald criteria
Yes. The McDonald criteria are a formal set of guidelines that have been regularly updated to help clinicians make an accurate MS diagnosis as early as possible. Depending on a person’s symptoms and test results, the help criteria outline which additional tests should be performed before confirming a diagnosis. Using these guidelines helps ensure MS is recognized quickly and accurately.
Dissemination in time means that nerve damage typical of MS has occurred at different points in time. Meanwhile, dissemination in space means that the damage has occurred in multiple parts of the central nervous system, which includes the brain, spinal cord, and optic nerves. These two findings can be used together or in combination with other MS-specific features to help doctors establish a diagnosis.
Yes, relapses are an important clinical feature that can help fulfill the McDonald criteria. For example, if a person has experienced two or more relapses, they have evidence of inflammatory activity occurring at multiple points in time, thereby meeting the criteria for dissemination in time.
Yes. Optic neuritis, which refers to inflammation in the nerves that carry information from the eyes to the brain, can be used to support an MS diagnosis under the 2024 McDonald criteria. The optic nerves are now one of the five regions considered when assessing dissemination in space, making optic nerve involvement an important clue that supports an MS diagnosis.
The 2024 update aims to help doctors confirm an MS diagnosis sooner while reducing the risk of misdiagnosis. Major changes include recognizing the optic nerve as an additional region for assessing dissemination in space, new guidance on specific MRI findings and test results, and introducing a single, unified framework to diagnose all types of MS and all age groups, replacing the separate criteria used previously. Importantly, these updates do not invalidate diagnoses made under earlier versions of the criteria.