MS relapses: Treatment and management
Last updated July 9, 2024, by Marisa Wexler, MS
 Fact-checked by Ines Martins, PhD
Fact-checked by Ines Martins, PhD
The vast majority of people with multiple sclerosis (MS) experience relapses, periods when existing MS symptoms suddenly worsen or new symptoms appear. These attacks alternate with remissions, periods when symptoms ease or go away entirely.
MS is a disease involving inflammation in the central nervous system — the brain and spinal cord — that damages myelin, a fatty sheath around nerve fibers.
Relapses are a defining hallmark of relapsing-remitting MS, the most common form of MS. These periods of symptom worsening also may be experienced by people with progressive types of MS, including primary progressive MS and secondary progressive MS.
What is an MS relapse?
According to the 2017 revisions to the McDonald criteria, a set of guidelines to help diagnose MS, a relapse occurs when new symptoms appear or existing ones worsen for 24 hours or more and cannot be explained by other factors such as a change in body temperature or infection.
These symptoms also must occur at least 30 days after the last relapse to be considered a distinct relapse.
There is no difference between a MS flare and a relapse — they describe the same clinical event. MS attack, flare-up, exacerbation, or episode are some other terms used to describe relapses.
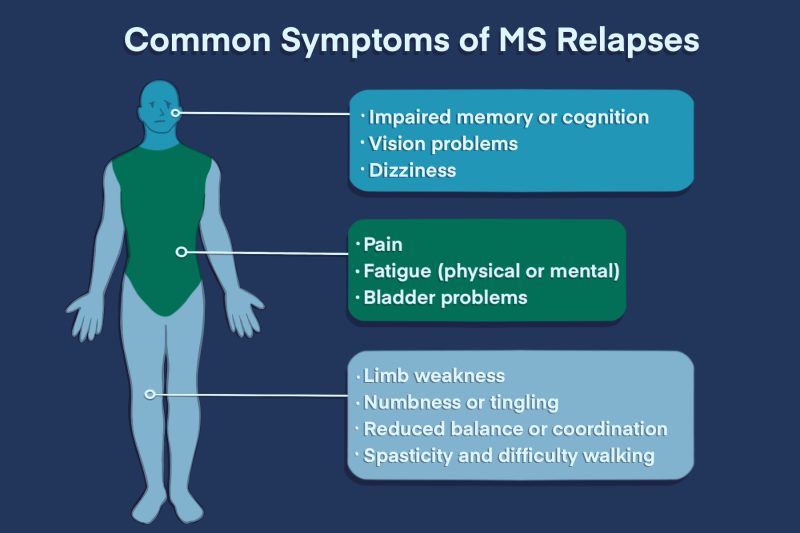
Common symptoms of MS relapses
Each person with MS will experience different symptoms during an MS relapse. The severity and frequency of MS relapses also can vary person to person, and even in the same individual.
Some relapses may cause severe problems in day-to-day life or require being treated in a hospital. Others might be mild enough to be managed at home.
MS relapse symptoms generally depend on the specific parts of the central nervous system that are being damaged by the immune system, but any MS symptom may appear or worsen during a relapse.
The most common symptoms and signs of an MS relapse include:
- fatigue
- pain
- numbness, tingling, or other unusual sensations
- dizziness
- difficulty with balance and coordination
- problems with memory and cognition
- vision problems
- weakness
- spasticity and difficulty walking
- bladder problems.
Multiple Sclerosis News Today columnists have described their experiences with MS flare-ups in different ways, such as:
- “The skin on my hands has been tight, tingly, and a little numb, while the rest of my body has felt numb on the surface of the skin,” Jessie Ace wrote.
- “My first symptom was facial numbness and blurred vision,” Beth Ullah wrote.
- “During the attacks my body seized up and I was unable to walk. My legs were so weak they would give out. My body was inflamed and everything was on fire with cramping and soreness. My usual fatigue was quadrupled. My strength was gone and I felt helpless,” Debi Wilson wrote.
How long does an MS relapse last?
Signs of an MS flare-up usually come on quickly, within hours or days.
To be considered a true relapse, the symptoms need to last for at least 24 hours. But the exact duration of a relapse depends on the severity of symptoms as well as what MS treatments are given.
Relapses usually last for about four weeks, although they can be as short as only a few days or as long as several months. When a relapse causes significant disability, anti-inflammatory medications such as glucocorticoids are often given.
Causes and triggers of MS relapses
Relapses are caused by new or worsening inflammation in the nervous system, which results in acute damage to nerves and gives rise to symptoms.
Exactly what causes this inflammation and triggers MS flare-ups is still not completely understood, but several factors are known to alter the risk of relapse.
Infections
Serious infections can trigger an MS relapse. They also can cause a pseudo-relapse, which is when symptoms temporarily worsen due to an increase in body temperature (fever). Infections in people with MS should be treated promptly.
Because vaccines can prevent infections and have not been shown to increase relapse risk, it’s generally recommended people living with MS receive all recommended vaccines.
Smoking
Smoking cigarettes has been linked to an increased relapse risk. MS patients who smoke also tend to experience more disabling symptoms during a relapse and take more time to recover from them.
Smoking also can indirectly affect relapse risk by increasing susceptibility to respiratory infections. MS patients who smoke are advised to quit.
Pregnancy
MS relapses tend to be less frequent during pregnancy, especially during the third trimester. However, relapse risk increases in the period immediately after childbirth. Overall, pregnancy does not change the overall course of MS.
Does stress increase relapse risk?
Many people with MS have anecdotally reported stress as a trigger for their relapses. Some studies have suggested a link between stress and a greater relapse risk, but other research has shown little or no connection.
Does alcohol increase relapse risk?
Drinking alcohol may worsen some MS symptoms, including cognitive impairment, depression, balance difficulties, and bladder problems. But there’s not a clear connection between drinking alcohol and relapse risk in MS.
Does heat increase relapse risk?
Many people with MS experience heat intolerance, where MS symptoms become more severe when body temperature increases, such as when exercising or in hot weather. This is sometimes called a “pseudo” (false) relapse, which is different from a relapse.
In an actual relapse, inflammation is causing new damage to the nervous system and symptoms last until the inflammatory attack is over.
In contrast, heat intolerance occurs because changes in temperature can alter how fast nerves are able to send electrical signals. Because nerves have already been damaged by MS inflammation, they are more sensitive to heat-related issues, which can result in a temporary worsening of symptoms. Symptoms usually go away once the person has cooled down.
Is there a way to prevent MS relapses?
The most well-established approach for preventing MS relapses is the use of disease-modifying therapies (DMTs), which can reduce the frequency of relapses and slow disease progression. In the U.S., more than 20 DMTs have been approved to treat relapsing forms of MS.
By reducing inflammation, DMTs can reduce disease activity and prevent new neurological damage. However, they cannot repair existing damage, so starting on a DMT as early as possible is critical to improving future outcomes.
Other ways to help reduce the risk of a flare-up include avoiding known triggers of MS relapses. Lifestyle changes to keep the body healthy also may help minimize relapse risk. Some general advice to prevent relapses includes:
- getting all recommended vaccines
- taking proactive steps to avoid infections, such as regular hand-washing and avoiding contact with people who have contagious illnesses
- exercising regularly
- eating a well-balanced diet
- getting enough sleep
- managing stress
- avoiding cigarettes, alcohol, and other drugs that may stress the body.
Do MS relapses go away on their own?
MS flare-up symptoms usually ease on their own without treatment, though the timing of recovery varies widely. It may take days, weeks, or months. Factors such as the severity of the relapse, the specific symptoms, and a person’s overall health can influence MS relapse duration.
Some available treatments can reduce the severity and duration of an MS flare-up, but these medications are generally given only when symptoms are severe.
After a relapse, most patients will have some lessening of symptoms, but MS relapse recovery is not always complete. In other words, some people will experience symptoms during a relapse that will continue to linger even after the relapse itself has resolved. An incomplete recovery is observed in about one-third to half of all relapses overall and is generally associated with a poorer prognosis of MS.
MS relapse treatment
While disease-modifying therapies and lifestyle adjustments can help reduce the frequency of relapses, most MS patients will experience occasional MS exacerbations that may require management with specific medications.
How do you calm an MS relapse?
No two MS relapses are exactly the same, and how they are managed is based on the needs of the individual. Some flare-ups may be mild enough that little or no additional support in day-to-day life is needed.
Other episodes may involve more debilitating symptoms, such as loss of vision, severe weakness, or problems with balance, and may require hospitalization.
Severe relapses may need MS relapse treatment, which aims to reduce the acute inflammation driving symptoms. This can speed recovery from relapses and also reduce their severity.
Glucocorticoids
Glucocorticoids, a class of corticosteroids, are usually the first line of treatment for severe MS relapses. These are powerful anti-inflammatory medications that work by mimicking the activity of cortisol, a naturally occurring hormone that suppresses the immune system. Glucocorticoids commonly used to treat MS relapses include:
ACTH-based therapies
When people with MS do not respond well or cannot tolerate corticosteroids, therapies containing a purified form of the adrenocorticotropic hormone (ACTH) can be used as an alternative relapse management approach.
These therapies stimulate the production of cortisol and other hormones in the body. Two products containing a purified preparation of ACTH are approved for managing MS relapses in the U.S.:
- Acthar Gel (repository corticotropin injection)
- Purified Cortrophin Gel (repository corticotropin injection).
Plasma exchange
Plasmapheresis, or plasma exchange, is sometimes considered when a person with MS is not adequately responding to corticosteroid therapy.
The procedure involves removing and replacing a person’s plasma — the liquid portion of blood — to eliminate antibodies and other molecules that may be contributing to the inflammation driving MS exacerbations.
When should you see a doctor for an MS relapse?
When people with MS suspect they’re having a relapse, they should contact their healthcare team to discuss possible triggers and any next steps for managing it.
If symptoms are causing substantial problems in day-to-day life, getting prompt medical attention is recommended.
Because relapses can be common when living with MS, some care teams provide more detailed instructions about what to do during a relapse. For example, some institutions have relapse clinics for MS patients or a phone number to call in case of suspected relapses.
Multiple Sclerosis News Today is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
FAQs about MS relapses
“MS relapse” and “MS flare-up” can be used interchangeably. Both refer to a sudden worsening of multiple sclerosis (MS) symptoms that cannot be explained by fever or infection. Other terms such as attack, clinical episode, and exacerbation also describe an MS relapse.
The biological causes of relapses in multiple sclerosis (MS) are not completely understood, but generally speaking, relapses are driven by new or worsening inflammation that damages nerves in the brain and spinal cord. This can interfere with nerve signals and ultimately lead to new symptoms or the worsening of older ones.
Some multiple sclerosis (MS) relapses are mild enough that they do not require treatment. Others may be severe enough to cause significant impairment and require urgent or emergency care. If patients think they are experiencing a relapse, they should contact their healthcare team to determine what to do.
Multiple sclerosis (MS) relapses can cause any of the wide range of symptoms that may occur in MS. The specific symptoms depend on which parts of the nervous system are being actively damaged. It can be different for everyone, and even from relapse to relapse for the same person. Some of the most common relapse symptoms include fatigue, pain or other unusual sensations, weakness, spasticity, difficulty with coordination or cognition, bladder problems, and vision difficulties.
Some people with multiple sclerosis (MS) are particularly sensitive to changes in body temperature and may experience a temporary worsening of symptoms called a pseudo-relapse. While it may feel similar to an MS relapse, it is not a true flare-up because symptoms are not caused by active inflammation, and resolve once body temperature returns to normal.