Does the myelin sheath play a role in MS?
 Fact-checked by
Fact-checked by
Multiple sclerosis (MS) is a disorder in which the body’s immune system attacks healthy parts of the central nervous system — the brain, spinal cord, and optic nerves. This inflammatory attack causes damage to the myelin sheath, a critical part of nerve cells.
What is the myelin sheath?
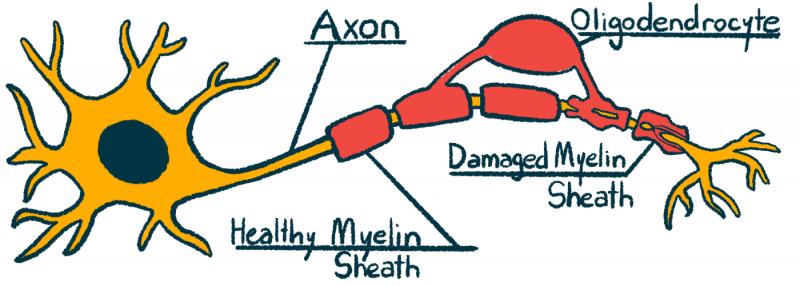
Nerve cells, known as neurons, are the cells in the nervous system responsible for sending electrical signals that govern body movements and give rise to thoughts and emotions. Each neuron contains a long fiber-like projection, called an axon.
When a neuron “fires,” an electrical current travels from one end of the axon to the other. Once it reaches the end, the electrical impulse triggers the neuron to release chemical messengers called neurotransmitters to pass the signal to other cells (for example, prompting a muscle to contract).
The myelin sheath is a coating surrounding axons, which are the nerve fibers. It is composed mainly of fatty molecules (lipids), as well as a number of specialized proteins. The sheath has a characteristic structure, with regions densely wrapped in myelin interspersed with areas of little to no myelin (referred to as the nodes of Ranvier).
In addition to neurons, the nervous system also is home to a diverse class of cells called glia, which play a number of roles to support neuronal function. Myelin in the central nervous system is primarily made by glial cells called oligodendrocytes.
How does the myelin sheath function?
The most well-characterized role of the myelin sheath is in helping neurons to send electrical signals faster. Conceptually, the myelin sheath wrapped around an axon is a bit like insulation coating a metal wire — just as rubber around a copper wire helps to insulate and direct electricity through the wire, myelin helps insulate and direct electrical signals through nerves.
The biophysics of this process are complicated and not entirely understood, but myelin’s structure is known to play a key role. When an axon does not have myelin, an electrical impulse needs to travel down the entire length of the axon in one go. By contrast, when an axon is wrapped in myelin, electrical signals can “skip” across the segments of dense myelin and travel across the areas with less myelin (the nodes of Ranvier), allowing the signal to travel faster.
It was long thought that this electricity-enhancing effect was the only role of myelin, but in recent years, research has shown that the myelin sheath actually has numerous other functions helping to maintain neuronal health. For example, the myelin sheath helps to support the metabolic activity of nerve cells, and it is important for regulating salt and water levels in the cell.
How is the myelin sheath linked to MS?
In MS, the immune system launches an inflammatory attack in the central nervous system. This inflammation leads to demyelination — the deterioration and loss of the myelin sheath — and causes damage to axons. Consequently, this leads to the development of lesions in the central nervous system where the tissue is damaged and scarred.
These lesions, which can be visualized on MRI scans, are actually how MS gets its name: The disease is characterized by “multiple” areas of scarring, or “sclerosis.”
MS is one of the most common demyelinating disorders that affect myelin in the central nervous system. As a result of this damage, nerve cells are not able to send electrical signals as efficiently; this impaired neuronal activity is mainly responsible for the symptoms of MS.
What causes damage to the myelin sheath?
It is not known exactly what prompts the start of the inflammatory attack that drives MS, and many interconnecting risk factors — including genetics, lifestyle habits, and environmental exposures — are known to contribute to the development of the disease.
The inflammatory attack itself involves the activity of many types of immune cells, including T-cells and B-cells.
- T-cells are immune cells equipped with specific receptors that can recognize a single molecule (usually a piece of a virus or bacteria). MS is commonly characterized by inflammatory T-cells, which are autoreactive against components of myelin.
- B-cells are best known as the cells that make immunological proteins called antibodies or immunoglobulins. It is common for people with MS to have high levels of antibodies in their cerebrospinal fluid (the liquid around the brain and spinal cord), and testing for these antibodies — a procedure called oligoclonal banding — may help in diagnosing MS.
Other immune cells involved in the MS-driving attack include dendritic cells and macrophages, which can secrete signaling molecules that promote inflammation. Dysregulated activity of glial cells, including microglia and astrocytes, also is involved in the attack.
Does the myelin sheath regenerate?
If myelin is damaged or destroyed, it can be repaired or replaced — a process referred to as remyelination.
Remyelination is done mainly by myelin-making oligodendrocytes, including mature oligodendrocytes that reside in the nervous system and new oligodendrocytes generated via the activation of immature cells called oligodendrocyte progenitor cells (OPCs).
While myelin repair in the body is possible, it is not very efficient — remyelination generally decreases with increasing age, and the inflammation that drives MS can further interfere with the process.
Finding therapeutic strategies that can promote remyelination is an ongoing area of research. Dozens of potential remyelinating treatments have shown promise in laboratory studies, and a few medications have shown positive results in early clinical studies in people with MS or other conditions associated with myelin loss.
Some of the potential remyelinating treatments being tested in MS clinical trials include:
A number of disease-modifying therapies have been developed for MS, mainly to reduce ongoing inflammation. Whether some of these medications also may act to promote myelin repair is still debatable.
Multiple Sclerosis News Today is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
FAQs about the myelin sheath and MS



Multiple sclerosis is caused by inflammation in the central nervous system, comprised of the brain, spinal cord, and optic nerves. This inflammation causes damage to nerve cells and results in demyelination — the destruction and loss of the myelin sheath, the protective coating around nerve fibers. Such damage to the central nervous system mainly is responsible for the symptoms of the disease.
Myelin damage in people with multiple sclerosis can be detected by MRI scans. On these imaging scans, areas of myelin damage and inflammation appear as lesions. There are several types of advanced MRI techniques and analytical strategies that can be used to assess damage to the myelin sheath. These include: magnetization transfer (based on the use of radiofrequency pulses to estimate myelin content); myelin water fraction imaging (based on the production of myelin water maps — by looking at water molecules “trapped” between the layers of myelin sheath — to assess myelin status/content); and diffusion tensor imaging (a technique to estimate myelin content based on tissue structure information obtained by measuring water diffusion).
The myelin sheath is needed for nerve cells to efficiently send electrical signals. If myelin is damaged or destroyed, the normal flow of these signals is interrupted and may lead to symptoms. The specific symptoms arising from damaged myelin depend on where the damage has taken place. For example, damage to the optic nerves (that connect the eyeballs to the brain) may result in visual symptoms, whereas damage in nerve cells of the spinal cord is commonly linked with motor symptoms, sensory problems, and trouble controlling the bladder and bowels.
It is possible for the body to repair a damaged myelin sheath. This process is led mainly by myelin-producing cells called oligodendrocytes. However, myelin repair is not a very efficient process in patients with multiple sclerosis. Thus, finding ways to promote better myelin repair is an active area of research.
B12 is a vitamin that is necessary for maintaining the health of the myelin sheath. Abnormally low B12 levels may cause MS-like symptoms. However, there is no robust evidence to support that B12 supplements provide additional benefit to patients with multiple sclerosis who have normal levels of the vitamin.
Related Articles