MRI and MS diagnosis
 Fact-checked by
Fact-checked by Magnetic resonance imaging (MRI), which produces detailed images of structures and tissues within the body, is the preferred imaging modality for assessing brain and spinal cord damage in multiple sclerosis (MS).
MS occurs when the immune system mistakenly attacks myelin, the protective coating around nerve cells, in the central nervous system, which includes the brain and spinal cord. This leads to inflammation and areas of damage known as lesions.
MRI can detect these lesions and reveal other signs of MS-related damage, making it the main imaging test used to confirm an MS diagnosis and monitor the disease over time.
How is MRI used to detect MS?
MRI is the most sensitive imaging technique for detecting MS lesions. It plays a central role in diagnosing MS and tracking disease progression.
Unlike an X-ray, which relies on radiation, the technique uses powerful magnetic fields and radio waves to measure water content in the body’s tissues. This works because water, which makes up much of the human body, contains subatomic particles that respond to the magnets.
Because myelin is fatty, it repels water. But areas where myelin has been damaged or lost cannot repel water as efficiently. The increased water content in these regions can appear as bright or dark spots on MRIs, depending on the type of scan.
MRI scans can be used across all MS types.
1. Diagnosing MS with MRI
During the diagnostic process, doctors may order MRIs of the brain and different parts of the spine, including the:
- cervical spine (neck region)
- thoracic spine (mid-back)
- lumbar spine (lower back)
Scans may also focus on the optic nerve, which carries signals between the eyes and the brain and is commonly affected in MS.
Radiologists examine these MRIs to identify features consistent with MS, including:
- dissemination in space: lesions in multiple areas of the central nervous system
- dissemination in time: evidence of lesions that formed at different points in time
- characteristic MRI features: specific patterns of lesions that are strongly linked to MS
These features are part of the formal guidelines for diagnosing MS, known as the McDonald criteria. Depending on the situation, other tests may be needed to confirm the diagnosis.
2. Measuring MS disease progression with MRI
After an MS diagnosis, patients will typically undergo routine follow-up scans to track disease progression and evaluate how well treatments are working.
The interval between these scans may vary depending on disease status, but doctors often recommend a scan within 3-6 months of starting a new therapy, and another scan 6-12 months later. Scans can then be done annually for most patients, though longer intervals may be considered for those with stable disease, and shorter intervals will generally be considered for patients with very active disease.
MS MRI results can help track the development of new lesions and monitor their location, size, number, and characteristics, providing relevant information about a person’s prognosis and helping guide treatment decisions.
In addition, scans can be used to assess brain atrophy in MS — the gradual loss of brain volume over time — which generally occurs at a faster rate in people with MS and can also inform prognosis.

Living with MS
Mental health and MS
Living with MS
Symptoms of MS vision problems

Living with MS
High-dose vitamin D delays MS progression
Does early MS show up on an MRI?
MS lesions are generally visible on MRI from the earliest stages of the disease, and they may even be apparent before a person experiences any MS symptoms.
When scans show MS-like lesions but diagnostic criteria are not fully met, doctors may diagnose one of two conditions:
- clinically isolated syndrome (CIS): the person has experienced one episode of MS-like symptoms
- radiologically isolated syndrome (RIS): the person has not experienced MS symptoms, but MS-like lesions were detectable on scans done for another reason
Not everyone with CIS or RIS will go on to develop MS, but follow-up MRIs can help monitor for changes over time and allow for a faster diagnosis among those who will eventually develop the condition.
Normal brain MRI vs. MS MRI
The main difference between a normal MRI and one from a person with MS is the presence of lesions, which represent areas of myelin loss (demyelination) and nerve cell damage (neurodegeneration). These lesions are usually visible as bright spots on MRI, but some types of scans show lesions as dark spots instead.
Below is a brain MRI scan from a young person with MS, which shows several lesions as white spots.
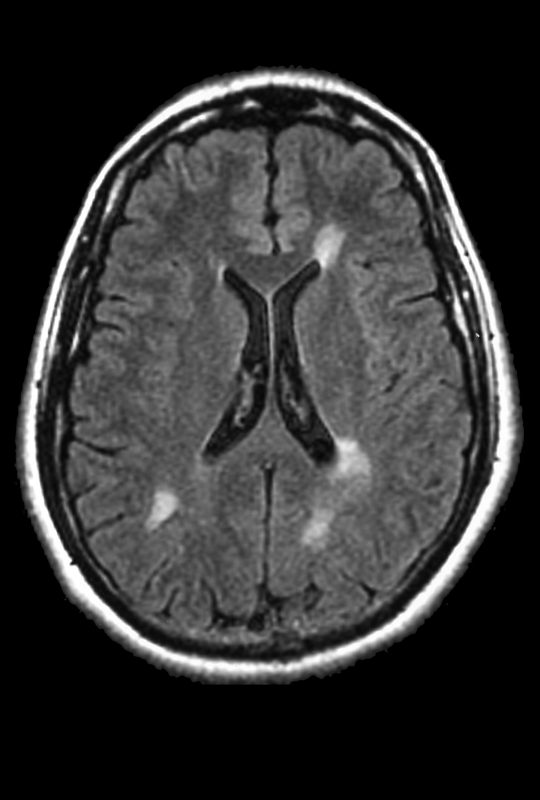
Image from a brain MRI of a young MS patient. The white spots correspond to demyelinating lesions. (Photo from ISM/SOVEREIGN)
While demyelinating lesions can also be found in conditions other than MS, some lesions have features that may help distinguish MS from other causes of brain damage. These include:
- central vein sign: a small vein running through the center of a lesion
- paramagnetic rim lesions: lesions with a dark rim around their edge that signals chronic inflammation
Proper interpretation of MRI scans requires training and expertise, so patients should always discuss the results with a qualified medical professional.
Can you have a clear MRI and still have MS?
MRI is one of the most sensitive tools for detecting lesions and is a cornerstone of MS diagnosis. The vast majority of patients have detectable lesions on MRI scans, but very small or early lesions may not always be visible.
In the earliest stages of the disease, an initial MRI may appear normal or nearly normal, especially if only the brain is scanned. For this reason, doctors often repeat MRI scans over time and may include the spinal cord or optic nerves to look for new or previously unseen lesions.
If high-quality MRI scans remain normal and other tests do not show signs of central nervous system inflammation, a diagnosis of MS becomes unlikely. In these cases, doctors will look for other possible causes of a person’s symptoms.
What are the different types of MRI scans for MS?
There are different MRI scans that can detect distinct aspects of MS-related damage. Some scans are done with a contrast agent called gadolinium, which is injected into a vein before the scan, to help show areas of active inflammation.
Normally, gadolinium cannot cross the protective barrier around the brain and spinal cord. But when inflammation is present, this barrier becomes more permeable, allowing the contrast agent to enter the tissue and be detected on MRI scans.
The most common types of MRI scans used in MS include:
- T1-weighted scans with gadolinium enhancement: show bright spots indicating lesions with active inflammation
- T1-weighted scans without gadolinium enhancement: show dark spots known as “black holes,” indicating areas of permanent nerve damage
- T2-weighted scans: show overall lesion burden, including active and inactive lesions
- T2-weighted FLAIR sequence: improve lesion detection by suppressing interference from the spinal fluid
The difference between T1- and T2-weighted scans depends on when the image is taken after the magnetic pulse. Patients should ask their healthcare team which types of scans will be used and what to expect during an MS MRI.
Is MRI safe for MS patients?
MRI scans do not use radiation and are generally considered safe. However, because scanners use powerful magnetic fields, they may cause metal objects to move rapidly or to heat up significantly.
For this reason, patients should not wear any metal during the scan. People with certain devices or internal metallic objects — such as pacemakers, cochlear implants, prosthetic devices, brain stimulators, and bullets or shrapnel — may not be able to undergo MRI scans.
Many newer medical devices are MRI-compatible, so patients should discuss their specific situation with their doctor. Pregnant individuals may also want to talk with their healthcare provider before undergoing an MRI.
People with claustrophobia or anxiety may find MRI scans uncomfortable. In some cases, a sedative for MRI may be used. An open MRI may be an option, though these machines often produce lower-resolution images and may be less suitable for detecting MS lesions.
Gadolinium contrast agents are generally considered safe, but they may carry risks for people with impaired kidney function and those who are pregnant. Gadolinium may also accumulate in the brain and other tissues, and it isn’t entirely clear whether this leads to health problems in the long term.
Multiple Sclerosis News Today is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.