
 Discussion
Discussion
Managing fatigue with MS
Last updated Jan. 16, 2025, by Susie Strachan
 Fact-checked by Inês Martins, PhD
Fact-checked by Inês Martins, PhD
Fatigue from multiple sclerosis (MS) can be both physically and mentally overwhelming. It is one of the most common challenges in MS, affecting about 80% of people with the disease.
MS symptoms usually first appear in young adults between the ages of 20 and 40. The condition is about three times more common in women than men. And it can affect nearly every part of your life.
For many, fatigue is considered the single most debilitating symptom of MS. It often feels like an overwhelming sense of tiredness with no obvious cause that is different from ordinary fatigue after a busy day at work or intense exercise.
While coping with multiple sclerosis and fatigue can be challenging, MS treatments and lifestyle changes can help you better maintain your energy levels.
How fatigue affects people with MS
Extreme fatigue from MS can make it hard to focus and plan, interfering with your daily routines and responsibilities.
It also can affect your social life — it can be like having an invisible symptom that is hard to explain to others.
While the exact causes of MS-related fatigue aren’t fully understood, several factors may contribute to it. It can arise as a direct consequence of nerve cell damage, or can be secondary to MS treatments, other MS symptoms, or the stress of living with a chronic disease.
Multiple sclerosis fatigue symptoms go beyond the usual tiredness from having a hectic or active day. They can be much more severe and persistent.
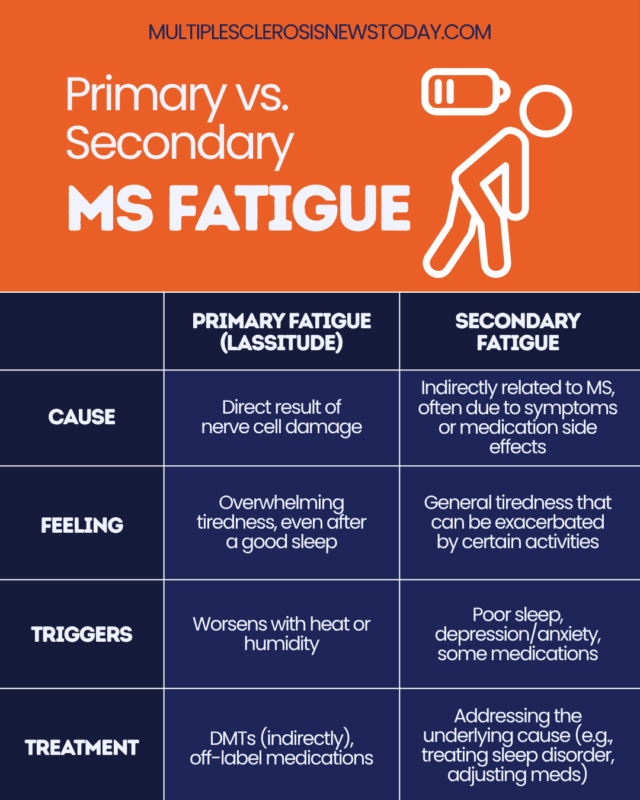
MS fatigue can be divided into two types: Primary fatigue is directly related to MS disease processes, while secondary fatigue can be from other factors related to MS, such as poor sleep or medication side effects. Knowing the difference can help you and your doctor find the right approach to managing it.
Primary fatigue, or lassitude, is thought to be caused by damage to the myelin sheath that insulates nerve fibers. It is different from ordinary tiredness, as it can start suddenly, be much more severe, and worsen with heat or humidity. You may still feel bone-tired even after a full night of restful sleep.
Secondary fatigue stems from factors indirectly related to MS. These may be complications from other symptoms, such as depression and emotional stress, or side effects from medications. Sleep disturbances, a common issue for people living with MS, can also contribute to secondary fatigue. For example, frequent nighttime urination caused by bladder dysfunction can disrupt sleep, leaving you exhausted during the day.
MS-related fatigue is different from chronic fatigue, which is a general feeling of overwhelming tiredness that isn’t linked to any one health condition.
Treating MS-related fatigue
Dealing with fatigue from multiple sclerosis can be overwhelming at times, but remember that your MS healthcare team is there to help. Let them know what is going on. Together, you can figure out how to regain some control over your energy levels.
Your doctor will first make sure that other possible causes of fatigue, such as anemia or sleep disorders like obstructive sleep apnea or restless legs syndrome, aren’t contributing to your tiredness. These issues tend to be more common in people with MS, so it’s important to rule them out.
Once those are treated or ruled out as a cause, your doctor will work with you to address your MS-related fatigue. This process may take time, and can require some trial and error to find what works best for you and your body.
Nondrug treatments for MS fatigue
There are several nondrug treatments that you might try to help manage your MS-related fatigue. These can include psychological interventions, which address your mental health and emotional well-being, and regular physical activity, which can support your overall energy levels.
Damage to the nervous system from MS can lead to mental health issues, such as depression and anxiety, which are more common in people with MS compared to the general population.
These mental health challenges can contribute to fatigue, as they can drain your energy and affect your overall sense of well-being.
Treatment options like cognitive-behavioral therapy and mindfulness-based cognitive therapy can help your emotional health. These therapies support you in managing fatigue by helping you change negative thought patterns, adopt healthier behaviors and sleep habits, and find relaxation techniques to relieve stress and conserve your energy.
Regular exercise can also play a role in managing fatigue. While it might seem counterintuitive to engage in physical activity when you’re already fatigued, exercise can improve your stamina, strengthen muscles, and improve sleep quality.
Following an exercise program, particularly one created by a physical or occupational therapist to fit your individual needs, can help you get the benefits without overexerting yourself.
MS fatigue drugs
Multiple sclerosis fatigue treatment also may involve medications.
There aren’t any medications specifically approved for MS fatigue, but your healthcare provider may consider using certain therapies off-label.
Certain stimulants and antidepressants may also be prescribed to manage MS-related fatigue.
Disease-modifying therapies, known as DMTs, are designed to slow the progression of MS and reduce disease activity. The treatments do not specifically target fatigue. But by managing the underlying disease and helping with MS symptom management, they may still have an indirect impact on fatigue and improve overall well-being.
Lifestyle changes to reduce fatigue
Small changes to your daily routine, habits, and self-care can make a real difference in managing fatigue and helping you feel more in control.
Energy conservation techniques
- Plan your day by tackling the most important tasks when you have the most energy.
- Break up tasks into smaller steps and stop and rest as needed to avoid overexertion.
- Don’t hesitate to ask for help with tasks.
Sleep hygiene
- Follow a regular sleep schedule to help regulate your body’s internal clock.
- Create a calming environment before bed by limiting screen time and engaging in relaxing activities like reading or listening to soothing music.
Managing heat sensitivity
- Stay cool by taking breaks in air-conditioned rooms or cooler areas.
- Wear lightweight clothing.
- Avoid activities in hot weather, such as walking in the heat.
Nutrition and hydration
- Eat a balanced diet of nutrient-dense, whole foods, such as leafy greens, berries, and whole grains, that provide long-lasting energy.
- Limit processed foods, sugary snacks, and high-fat foods that can lead to high-energy peaks and energy crashes.
- Drink plenty of fluids to stay hydrated, especially if you’re feeling fatigued.
Reducing stress
- Set aside time each day for relaxation practices like deep breathing, meditation, or gentle stretching.
- Break up your day with stress-reducing activities, such as listening to music, spending time in nature, or doing a hobby you enjoy.
- Use mindfulness techniques to avoid becoming overwhelmed by stress.
Daily tips
With a few simple tips, you can save your energy, stay on top of tasks, and avoid burnout from MS-related fatigue.
- Create a daily schedule with built-in breaks to help pace your activities and avoid overexertion.
- Set alarms throughout the day to remind you to rest or nap.
- Use tools that make daily tasks easier, such as a grabber for picking things up.
- Keep a fatigue diary or use an MS app to track your daily activities, and aid in identifying patterns or triggers that may add to your fatigue.
Multiple Sclerosis News Today is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related content
-
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion
-
 Discussion
Discussion