Managing the ups and downs of relapsing-remitting MS
Last updated Jan. 15, 2025, by Marisa Wexler, MS
 Fact-checked by Inês Martins, PhD
Fact-checked by Inês Martins, PhD
Relapsing-remitting multiple sclerosis, often referred to as RRMS, is the most common type of multiple sclerosis (MS). It is defined by relapses or flares, periods where new symptoms suddenly appear and/or existing symptoms suddenly get worse — followed by periods of remission where symptoms ease or disappear entirely.
RRMS is generally unpredictable. It’s impossible to know exactly when a relapse will occur or which symptoms you will experience during a relapse. While there are treatments that can lessen the frequency and severity of MS flares and to manage severe relapses when they occur, symptoms may still worsen even when you’re not having relapses.
For these reasons, managing RRMS is a lifelong task that requires understanding the medical aspects of the disease, as well as dealing with both the physical symptoms and the emotional challenges that come with MS. Doctors and other healthcare professionals can be an invaluable resource for figuring out how to manage RRMS. Patient organizations, support groups, and friends and family can also offer crucial support.
The effect of RRMS on the body
Like all forms of MS, RRMS is characterized by inflammation in the brain and spinal cord. The inflammation causes damage to myelin, a protective sheath around nerve fibers that’s critical for normal nerve signaling, which ultimately leads to MS symptoms.
People with RRMS experience relapses when there is new or worsening inflammation in the nervous system that causes new problems with nerve signaling. The relapse ends when the inflammation has been brought under control and the body was able to repair or compensate for the damaged regions.
During a relapse, existing symptoms may get worse or new symptoms may appear. Some relapses cause just one symptom, while others may involve multiple symptoms simultaneously. Your relapses may be completely different from another person’s experience, and your own relapses may also be different from one another.
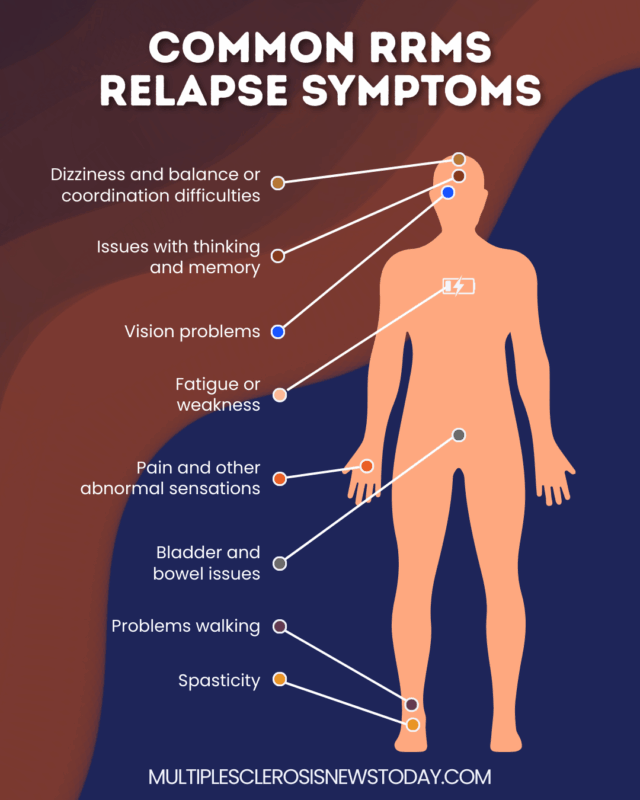
The most common RRMS symptoms that occur during a relapse include:
- fatigue or weakness
- pain or other unusual sensations such as numbness or tingling
- dizziness or other difficulties affecting balance and coordination
- issues with thinking and memory
- vision problems
- spasticity
- problems walking
- bladder and bowel issues.
After a relapse ends, your RRMS symptoms may disappear completely or you may experience an incomplete recovery with some lingering symptoms. This is particularly more common with relapses that occur later on in the disease course. Also, the remaining inflammation in the brain and spinal cord may continue to cause damage over time, leading to a gradual worsening of RRMS symptoms even when you don’t experience any relapses.
Recognizing and managing RRMS flares
Identifying and managing disease relapses are key aspects of living with RRMS. If you believe you’re having a relapse, you should contact your healthcare team to discuss the best course of action. Depending on the type and severity of your symptoms, your care team may decide to let the relapse subside on its own with minimal support or try treating it to reduce the underlying inflammation.
Signs
A relapse is defined by the appearance of new MS symptoms and/or the substantial worsening of existing ones over the course of a few hours or days.
To be considered a true relapse, sudden symptom worsening must meet three criteria:
- the symptoms last for at least 24 hours
- the symptoms occur at least 30 days after the start of the previous relapse, otherwise it’s considered a continuation of the prior relapse rather than a new one
- the symptoms are not explained by external factors, such as infections, stress, or a change in body temperature, that are known to cause a temporary worsening in MS symptoms.
If you are experiencing new or worsening symptoms that don’t have an obvious explanation, there’s a good chance you are experiencing a relapse. When in doubt, you should speak with a medical expert.
Treatment
When an RRMS flare occurs, MS relapse treatment may be given to help bring the relapse under control depending on the type and severity of symptoms. The specific treatment regime will be based on your situation.
When treatment is necessary for managing MS flares, it generally involves anti-inflammatory therapies that suppress the immune system to control relapse-driving inflammation. It can include:
- glucocorticoids, which are the first line of therapy for severe relapses
- ACTH-based therapies, which can be used if you don’t respond or tolerate glucocorticoids
- plasma exchange, which replaces the liquid portion of blood to remove antibodies and other molecules involved in MS inflammation, and can also be considered if your relapse does not respond well to steroid therapy.
In addition to anti-inflammatory treatments, you may benefit from medications that can ease specific MS symptoms and also from rehabilitation programs, such as physical therapy, occupational therapy, and speech therapy. These types of specialist interventions can also help you with making adaptations that support you in your daily activities if you are dealing with new long-term symptoms after the relapse has ended.
Lifestyle changes
Changes in lifestyle, such as eating a healthy diet, having good sleep habits, or exercising, won’t help end a relapse, but they may make it easier to manage symptoms during and after a disease flare. For example, if you are having spasticity or mobility issues, you may benefit from tailored exercise for RRMS, while a person struggling with mental health challenges or emotional changes might benefit from talk therapy.
The best RRMS exercise and therapy program for you will be based on your specific situation and needs. You should work closely with your care team to develop strategies for managing your specific symptoms.
Lifestyle changes can also help you avoid triggers that may increase the risk of a relapse. For example, serious infections can set off relapses in RRMS, so protecting yourself from infections, such as by getting all recommended vaccines, regular hand-washing, and staying away from people who have a contagious illness, may help to prevent relapses.
Smoking cigarettes is also known to increase the risk of relapse, so anyone living with MS is generally advised to quit or limit smoking.
Hormonal changes that occur during and after pregnancy also may act as RRMS flare triggers, so if you are pregnant or are planning to become pregnant, you are advised to talk to your care team about the best ways to try to minimize the risk of a relapse and stay healthy.
While there is data suggesting low vitamin D levels, emotional stress, and drinking alcohol may increase your chances of having a relapse, there isn’t definitive proof that any of these can act as RRMS flare triggers. Still, it’s generally advised that if you have RRMS you should try to minimize your intake of alcohol and other drugs, work on stress management, and get enough vitamin D.
Progression and long-term management
After a relapse, symptoms usually ease, and sometimes they disappear entirely, but it’s also possible that some symptoms won’t go away after a relapse and become permanent. This type of worsening is called relapse-associated worsening or RAW.
It’s also possible for someone with RRMS to experience worsening symptoms that occur without an obvious relapse. This is sometimes called “silent progression,” although it’s more formally known as progression independent of relapse activity or PIRA.
Both RAW and PIRA can contribute to RRMS progression and lead to symptom worsening over time. It’s important to minimize relapse risk and manage relapses appropriately when they occur. But it’s also vital that you have regular check-ups to evaluate if and how symptoms are worsening in the absence of relapses.
DMTs to modify disease progression
The long-term management of RRMS mainly involves medications known as disease-modifying therapies or DMTs that reduce the inflammation that drives MS.
Data suggest starting on DMTs for MS earlier is associated with slower disability accumulation over time. In other words, people with RRMS who start a DMT early on will often take longer to reach certain disability milestones, such as needing a walking aid or a wheelchair.
There are more than 20 DMTs approved in the U.S. for RRMS treatment. All have been proven in clinical trials to reduce the risk of relapses, but how well the drugs work varies.
Available DMTs can be broadly divided into two categories based on their efficacy:
- Moderate-efficacy DMTs, such as interferon and fumarate therapies, are not as effective at controlling MS relapses but generally have fewer side effects.
- High-efficacy DMTs, such as anti-CD20 antibodies and S1P modulators, are more powerful for preventing MS relapses, but also tend to have more substantial side effects and safety risks.
There is no one DMT that’s right for everyone. You should work with your care team to determine which DMT is most appropriate for your situation. Before deciding on a treatment, doctors will consider factors such as age and previous treatments, how active your RRMS is, and your own preferences.
In general, early treatment with a high-efficacy DMT is the best approach for delaying irreversible disability, but a moderate-efficacy DMT may be considered if you experience few relapses or are at a greater risk from side effects.
Conversion to SPMS
Over time, some people with RRMS will develop secondary progressive MS (SPMS), which is defined by symptoms that get gradually worse without any relapses. People with SPMS may still experience some relapses, but PIRA is the main driver of disability worsening in SPMS.
In the absence of MS treatment, roughly half of people with RRMS would progress to SPMS within a decade of disease onset. But with available DMTs, fewer than 1 in 10 people with RRMS will progress to SPMS. This transition also commonly happens several decades later with treatment.
While most RRMS treatments are also approved in the U.S. for SPMS, these therapies are only indicated for people who have active MS, or those who continue to experience relapses or have signs of active inflammation in the brain and spinal cord. It’s estimated that nearly three-quarters of people with SPMS will have a nonactive disease form, and very few treatment options are available for them.
RRMS life expectancy
MS itself is not a fatal disease. But the disease may increase the risk of life-threatening health complications, such as pneumonia and urinary tract infections.
Presently, the life expectancy for someone with MS is around five to 10 years shorter than it is for the general population. However, RRMS life expectancy tends to be higher than other forms of MS and closer to the general population. A Norwegian study that followed patients with MS for 60 years showed that those with RRMS lived for about 77.8 years, compared with 81.8 years for the general population.
With the recent introduction of highly effective DMTs and the development of new ones that are progressively better at treating MS, it’s expected that this gap will continue to narrow over time.
Living with RRMS
Living with RRMS can be challenging, but there are steps you can take to manage your disease and improve your well-being and quality of life:
- eating a well-balanced diet
- exercising regularly
- quitting smoking, limiting alcohol intake, and minimizing use of other recreational drugs
- taking all MS treatments as directed
- dealing with MS symptoms, which can involve medications for pain management or spasticity, as well as resting if fatigue becomes too severe
- managing any other co-occurring health conditions
- actively working on mental health and emotional wellness
- leaning on friends and family for support
- asking for help whenever needed.
Support groups and resources
There are many MS support groups for people living with RRMS. In the U.S., the National Multiple Sclerosis Society and the Multiple Sclerosis Foundation offer regular support groups for you and your loved ones. Support groups are also available in many other parts of the world, such as through the Multiple Sclerosis International Federation.
In addition to support groups, many of these patient organizations offer other resources including educational materials and financial assistance. Healthcare providers are often knowledgeable about local resources, so it’s always a good idea to ask them for recommendations.
In addition to in-person and logistical support, there are many online resources for people with RRMS. At Multiple Sclerosis News Today, you can access forums and a Facebook page to connect and share information with others living with MS, as well as find news about the most recent treatments and clinical trials and columns by people with MS and their caregivers.
Multiple Sclerosis News Today is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Related articles
-
-

-
 Discussion
Discussion
-

-

-